Pull a thread
to untangle the story
If you’re interested in hearing
more about the ST2/IL-33 pathway,
scan the QR code or speak to
a Roche representative.

© 2025 F. Hoffmann-La Roche Ltd. All rights reserved.
M-XX-00021326 | July 2025
M-XX-00021326 | July 2025
Explore
EXACERBATIONS
EXACERBATIONS
Explore
INFLAMMATION
INFLAMMATION
Explore
The ST2/IL-33
PATHWAY
The ST2/IL-33
PATHWAY
Reducing
exacerbations
is still a major
challenge in
the treatment
of COPD1,2
COPD is a chronic
respiratory disease
characterised by
progressive airway
inflammation...

...yet traditional therapies,
such as bronchodilators
and corticosteroids,
do little to target the
underlying biology.3–5
Every exacerbation
causes lasting lung damage,
contributing to disease
progression…
Pull the thread
...increasing a patient's risk of hospitalisation or death,
and significantly impacting a patient's ability to live their life.6-9
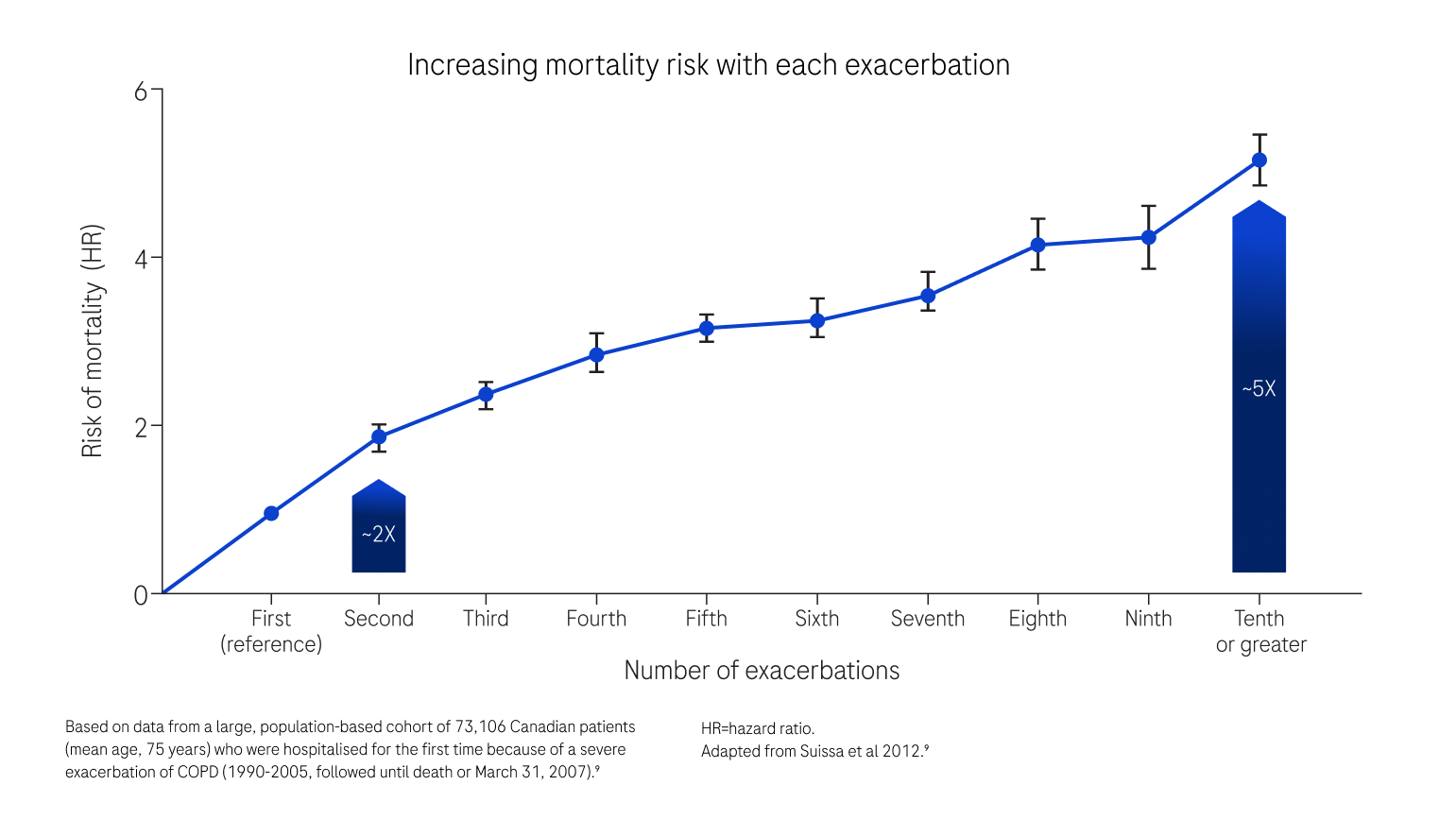
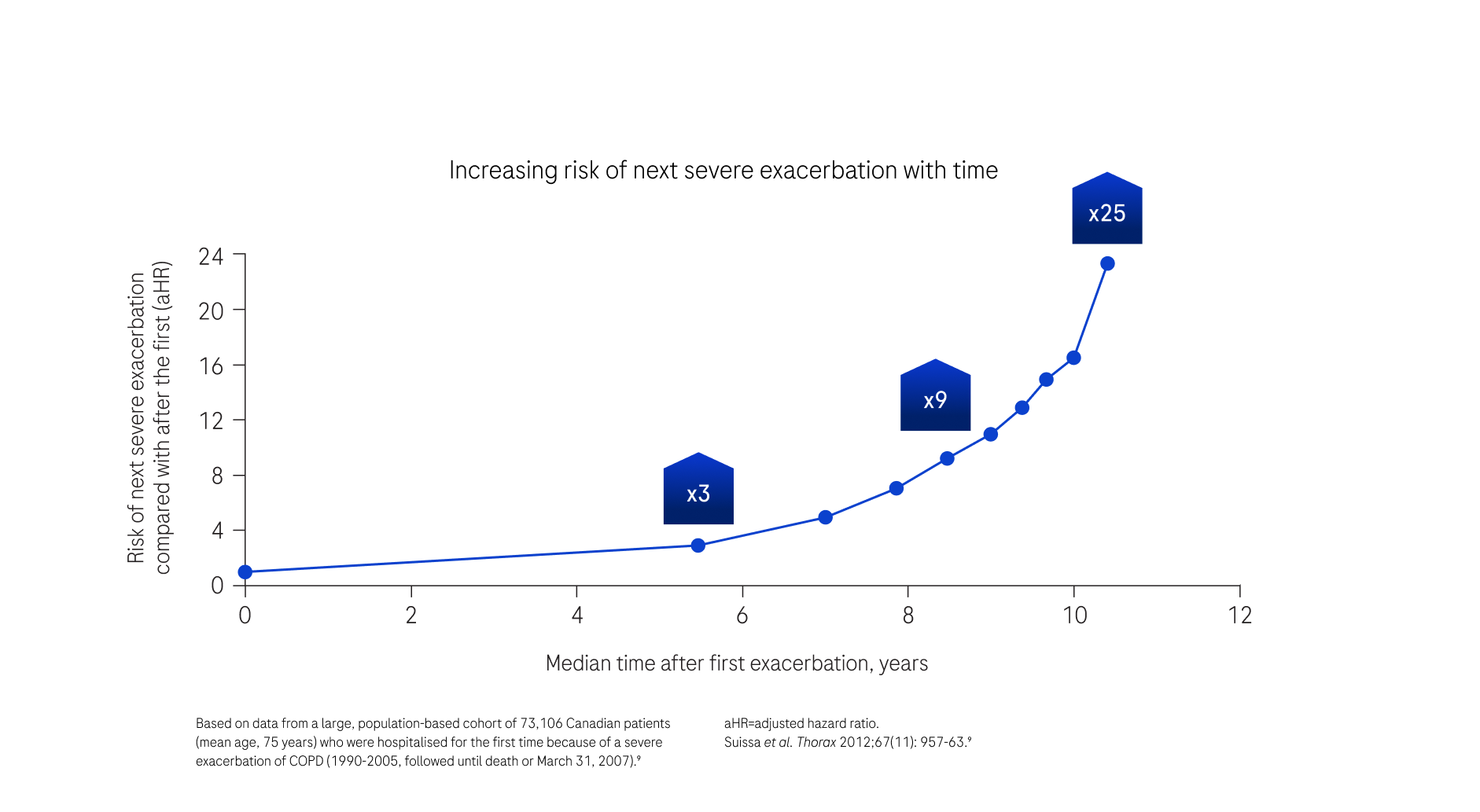
In addition, each exacerbation increases
the risk of the next exacerbation.9
51%
31%
21%
41%
51%
What percentage of
patients with a history of
exacerbations continue to
suffer from exacerbations?
Select from the
options shown
options shown
TRY AGAIN
CORRECT
Even with current
therapies, up to 51% of
patients with a history
of exacerbations
continue to suffer from
exacerbations10*
*moderate or severe.
Pull the thread
COPD is a
heterogeneous
disease4,11,12
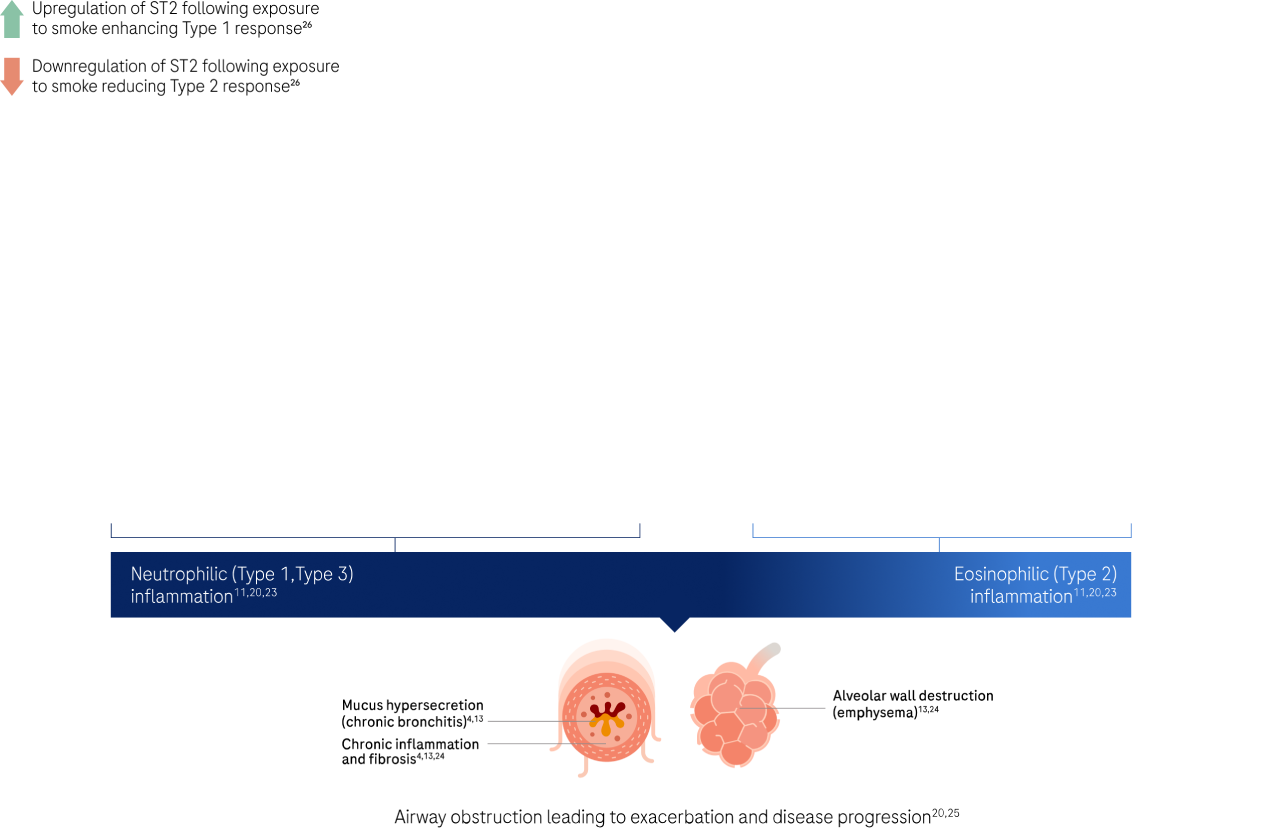
…with the presence of both
neutrophilic (Types 1 & 3)
and eosinophilic (Type 2)
inflammation.5,11–17
What do you currently believe to be
the predominant type of inflammation
in the majority of people with COPD?
A Eosinophilic inflammation (Type 2)
B Neutrophilic inflammation (Type 1, Type 3)
C Both in equal measure
Neutrophilic inflammation is the
predominant type, with the vast
majority of patients (up to 92%)
having airway neutrophilia.4,13,15-18
Neutrophilic inflammation contributes to extracellular matrix
degradation, fibrosis, emphysema and mucus hypersecretion,
leading to airflow obstruction and exacerbations.4,13

With its central role in
pathogenesis, it remains the
greatest unmet need in COPD
treatment.4,5,15-17
Pinch the threads
and pull them together
to continue
and pull them together
to continue
Understanding how we could address
neutrophilic inflammation as well as
eosinophilic inflammation…
...could be key to reducing
exacerbations across a broader
population of patients.5,13
ST2/IL-33 works
upstream to drive
both eosinophilic
and neutrophilic
inflammation12,19
Pull the
thread
thread
Following exposure to tobacco smoke, bacteria
and viruses, damaged lung epithelial cells release
a number of different alarmins, one of which is
IL-33 - an ST2 receptor-mediated cytokine.12,19
Pull the thread

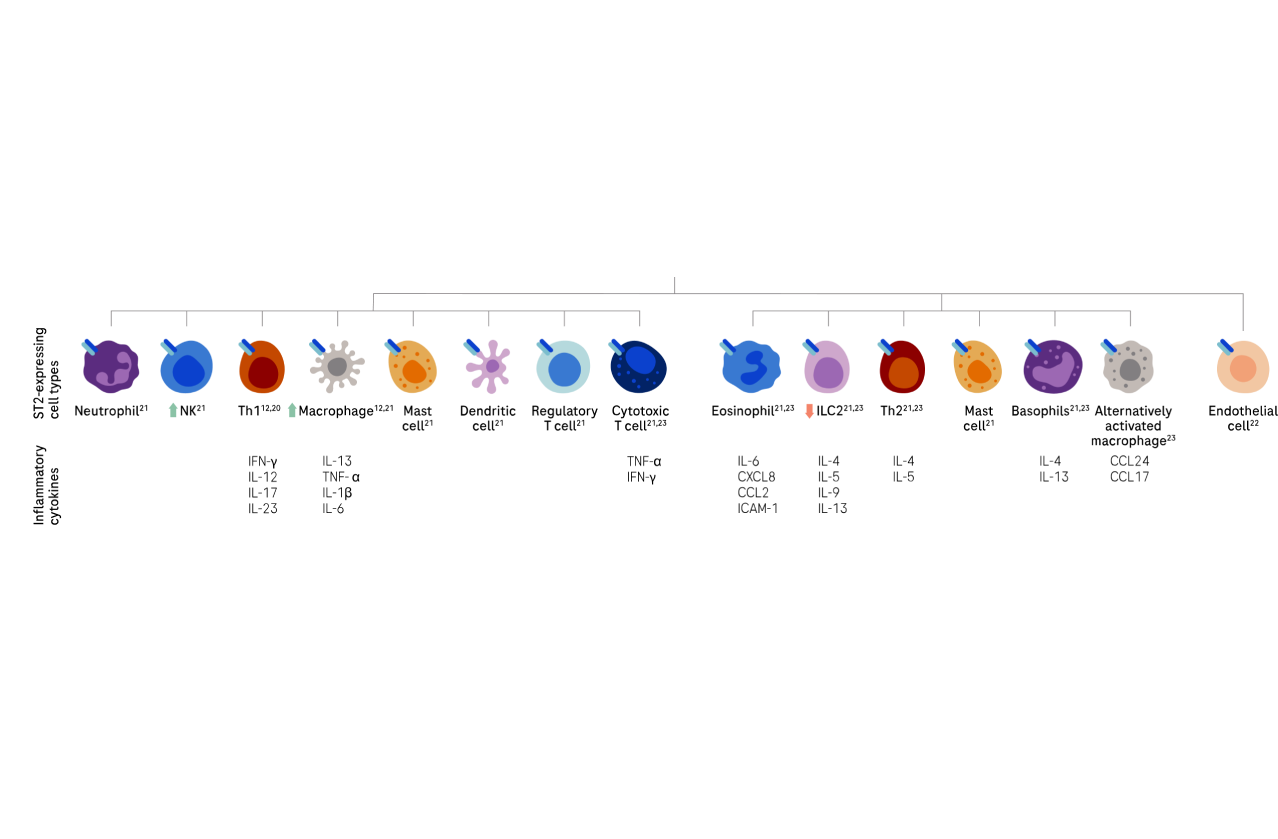
Binding of IL-33 to the
ST2 receptor, expressed
across a broad range of
immune cells
initiates and amplifies
multiple downstream
inflammatory pathways
that contribute to both
neutrophilic (Type 1 and 3)
and eosinophilic (Type 2)
inflammation12,19
Studies are investigating
the impact of targeting
the ST2 / IL-33 pathway
in a broad population of
COPD patients.27-33
Pull the thread